

Introduction: Relief of symptoms and splenomegaly are important treatment goals for all patients with myelofibrosis (MF). Until 2019, ruxolitinib (RUX) was the only FDA-approved therapy for the treatment of intermediate- or high-risk MF. This study sought to explore real-world treatment patterns and clinical outcomes, including spleen response, hematologic response, and patient symptomology during first-line (1L) RUX therapy to describe the unmet need in RUX-treated patients with MF.
Methods: A retrospective, multisite (US community oncology practices) medical chart review of patients with MF who initiated 1L RUX between January 2015 and December 2017 was undertaken. Patient demographic and clinical characteristics at initiation of RUX, and RUX dosing and dose modifications were abstracted. In addition, at the initiation of RUX and every patient visit during the first 6 months of therapy, physicians abstracted data on spleen size, symptom burden, and hematologic parameters. We assessed the rate of dose modifications (decrease or increase) during the first 6 months of therapy and subsequently compared patients who dose modified to those who did not (stable dose). Univariate comparisons between cohorts of baseline characteristics were performed (chi-square and t-tests). Time to treatment discontinuation was described. The proportion of patients with spleen length reduction, palpable spleen resolution, resolution of ≥ 1 baseline symptom, and platelet decrease to < 100 × 109/L at 6 months following RUX initiation was described and compared between dose-modified and stable-dose cohorts. The Kaplan-Meier method was used to estimate these proportions; patients were censored on their date of treatment discontinuation if the outcome had not occurred.
Results: Data for 152 patients were collected from 37 different sites across the USA (South 43.2%, Northeast 21.6%, Midwest 18.9%, West 16.2%). Mean follow-up was 26 months from initiation of 1L RUX; 29% of patients were deceased at the time of data abstraction. Overall, 69 patients (45.4%) were not initiated on the recommended dose of RUX based on their platelet count according to US package insert.
Forty-five patients (29.6%) were dose modified during the first 6 months of therapy including 39 with dose decreases and 7 with dose increases (1 patient had both a decrease and increase). Physicians reported the most common reason (76.9%) for dose reduction was a hemoglobin level of 8-10 g/dL or platelet count 50-75 × 109/L. The most common reason (57.1%) for dose increase was provider decision to start on a low dose and titrate to a therapeutic dose. Mean age at diagnosis was significantly higher in the dose-modified subgroup (70 vs 62 years, P < 0.01) compared to the stable-dose subgroup, while platelets at the time of RUX initiation were significantly lower (246 vs 326 × 109 /L, P = 0.03); no other baseline factors were associated with dose modification during the study period.
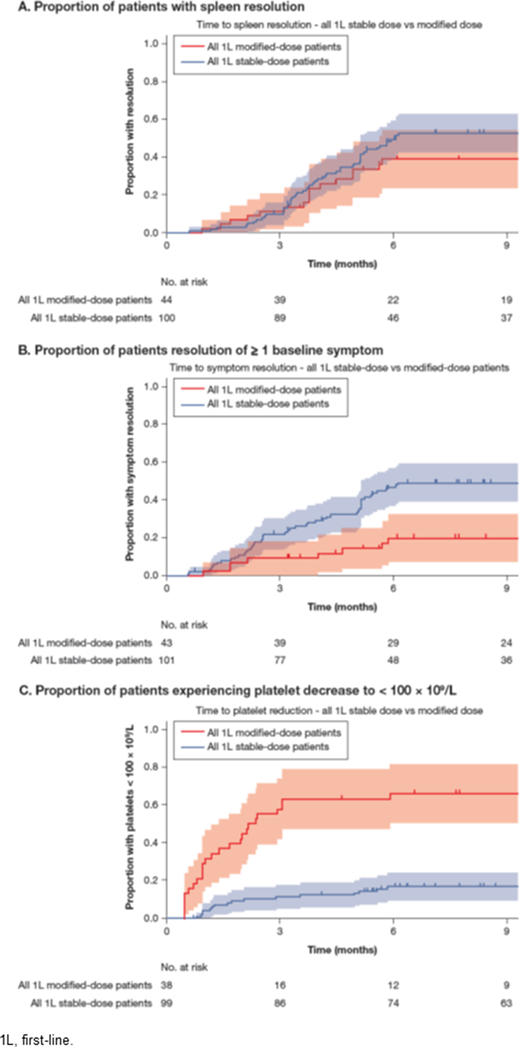
At the time of chart data abstraction, 57.0% of stable-dose and 66.7% of dose-modified patients had discontinued RUX. Among stable-dose and dose-modified patients who had discontinued RUX, the median time to discontinuation was 10.7 and 10.0 months, respectively, while duration of treatment for patients still receiving RUX was 26.4 and 28.6 months, respectively. At 6 months, while not statistically significant, a lower proportion of patients in the dose-modified cohort achieved spleen length reduction by palpation (57.9% vs 65.6%; P = 0.710) and resolution of splenomegaly (39.1% vs 49.3%; P = 0.090) (Figure, panel A). A lower proportion of patients in the dose-modified cohort had resolution of ≥ 1 baseline symptom (19.9% vs 39.1%; P = 0.003) (Figure, panel B). Among patients with ≥ 100 × 109/L platelets at baseline, a significantly higher proportion of patients in the dose-modified cohort had platelets decrease to < 100 × 109/L during 1L RUX treatment (66.0% vs 16.7%; P < 0.001) (Figure, panel C).
Conclusions: Dose modifications occurred in nearly one third of 1L RUX-treated patients, with the majority requiring a dose decrease. Patients with dose modifications were less likely to have improved splenomegaly or symptom burden and experienced significantly lower platelet counts than those who maintained a stable dose of RUX during the first 6 months of therapy. These findings identify a population of RUX-treated patients with a significant need for alternative MF treatments.
Kish:Cardinal Health: Current Employment, Current equity holder in publicly-traded company. Kee:Bristol Myers Squibb: Current Employment. Abraham:BMS: Current Employment, Current equity holder in publicly-traded company. Copher:Bristol Myers Squibb: Current Employment. Miller:Cardinal Health: Current Employment. Gerds:Imago Biosciences: Research Funding; Roche/Genentech: Research Funding; CTI Biopharma: Consultancy, Research Funding; Pfizer: Research Funding; Apexx Oncology: Consultancy; AstraZeneca/MedImmune: Consultancy; Sierra Oncology: Research Funding; Incyte Corporation: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Gilead Sciences: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal